

Introduction
Overview of KPV (ACTH(11-13), alpha-MSH) and its therapeutic properties
KPV is a peptide fragment derived from alpha-melanocyte stimulating hormone (alpha-MSH). This peptide has garnered attention for its potential photoprotective properties, efficacy against ischemia, impact on sexual function, and influence on feeding behavior and energy balance. Notably, KPV, composed of lysine-proline-valine, exhibits significant anti-inflammatory effects[1]. Researchers are actively exploring its therapeutic potential in managing inflammatory bowel disease, as it demonstrates potent anti-inflammatory properties in various bodily systems such as the central nervous system, gastrointestinal tract, lungs, vascular system, and joints. Due to its small size, KPV can be administered through multiple routes, including oral, intravenous, and transdermal methods.
Dosing & Reconstitution Guide
Educational guide for dosing, cycling, cautions, and vial-format options
KPV is described as a naturally produced peptide found in the hormone alpha-MSH. It’s most commonly discussed for autoimmune and inflammatory research contexts, with additional notes involving the central nervous system, gastrointestinal tract, lungs, vascular system, and joints.
Because KPV is a small peptide, it’s described as being usable as a cream, injectable, and/or capsule. The route of administration depends on the area being focused on.
Deeper Research Notes (Mechanism Summary):
• Described as targeting inflamed areas while minimizing impact on healthy tissues (including discussion of nanoparticle delivery to help carry KPV to inflammation sites).
• Described as entering cells and nuclei and inhibiting NF-κB, a key controller of inflammatory signaling.
• Discussed for lowering inflammatory markers like TNF-alpha, with research mentions related to conditions like IBD.
• Topical use is described for promoting wound healing and helping prevent scarring by inhibiting bacteria and fungi while supporting tissue repair.
Dosing & Cycling (As Listed):Note: Cycle length and intensity depend on response and goal.
| Protocol Item | Guidance |
|---|---|
| Dose | 200–500 mcg per dose |
| Cycling | Typical cycles are daily for 30 days, and may be extended to 90 or 120 days, with a 30-day minimum cycle break between cycles. |
Caution & Contraindications:
Caution:
• May cause headaches or nausea
Contraindications:
• Generally well tolerated based on current research (no specific contraindications listed)
Reconstitution Options (Vial Format):
• 4 mg
• 5 mg
Reconstitution (General Handling):
• Use sterile technique and sanitize the vial stopper before access.
• Add diluent slowly along the vial wall to minimize foaming.
• Gently swirl/roll until fully dissolved (avoid vigorous shaking).
• Choose a diluent volume that makes a 200–500 mcg dose easy to measure accurately.
• Store according to the product label/spec sheet and protect from light as applicable.
Structure
Molecular composition and structural details of KPV
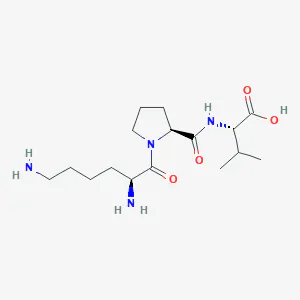
Sequence: Lys-Pro-Val
Molecular Formula: C16H30N4O4
Molecular Weight: 342.43 g mol−1
PubChem CID: 125672
CAS Number: 67727-97-3
Intestinal Inflammation
KPV’s effectiveness in treating inflammatory bowel disease
Research stemming from KPV investigations has uncovered its ability to mitigate intestinal inflammation significantly. In studies involving mouse models with inflammatory bowel disease (IBD), KPV demonstrated robust outcomes by reducing inflammatory infiltrates, MPO activity, and overall histological signs of inflammation. Compared to a placebo, mice treated with KPV exhibited accelerated recovery and more substantial weight gain. Additional exploration into KPV’s delivery methods has unveiled that loading KPV onto nanoparticles functionalized with hyaluronic acid can effectively target the peptide’s anti-inflammatory effects within the intestine. This approach leads to accelerated mucosal healing and the alleviation of inflammation, primarily through the strong down-regulation of TNF-alpha in mouse models. KPV, in this regard, offers a more effective and precise means of curbing IBD-related inflammation without affecting TNF-alpha levels elsewhere in the body. Modifying KPV aims to enhance its oral bioavailability, which doesn’t increase the peptide’s effectiveness but influences its potency, thus reducing the required total dosage for an effect.
Concentration
KPV’s mechanism of action and concentration-dependent effects
Research indicates that KPV’s impact extends beyond TNF-alpha inhibition; it also reduces NF-kappaB and mitogen-activated protein kinase activity. These effects complement TNF-alpha inhibition, collectively diminishing inflammatory changes in the intestine. Mice treated with KPV display significantly less colonic infiltration and normal colon lengths compared to control groups. Notably, the graph above reveals that KPV primarily exerts its effects in cases of heightened inflammation and has minimal impact on normal tissue. This phenomenon is attributed, in part, to KPV’s ability to enter colonic cells through a transporter that becomes upregulated during inflammation. Consequently, KPV may serve as an effective preventive or maintenance medication for IBD, even during quiescent periods, as it remains inactive unless needed and is excreted otherwise. Recent findings by Professor Didier Merlin suggest that KPV enters colonic cells via PepT1, a protein channel predominantly expressed in the intestine during inflammatory states. This explains KPV’s enhanced effectiveness in inflamed settings and hints at a novel drug delivery approach applicable to various conditions. By targeting proteins altered during disease conditions, it might be possible to concentrate drug activity in specific areas, potentially reducing dosages of drugs with severe side effects and developing therapeutics tailored to specific disease states.
KPV as a General Anti-Inflammatory
KPV’s broad anti-inflammatory effects across various conditions
Research as far back as 1984, involving rabbits, uncovered KPV’s potent anti-inflammatory and fever-reducing (anti-pyretic) properties. However, KPV demonstrated lower potency in this regard compared to the full alpha-MSH molecule. This observation prompted decades of research into modified forms of alpha-MSH. Collectively, these tests have highlighted that alpha-MSH and its analogues possess anti-inflammatory properties effective across a wide range of diseases. These molecules have undergone testing in fever, irritant and allergic contact dermatitis, vasculitis, fibrosis, arthritis, and inflammation in various organs, including the eyes, brain, lungs, and gastrointestinal tract. In all instances, alpha-MSH emerges as the most effective anti-inflammatory agent. Unfortunately, it also induces skin pigmentation as a major side effect. KPV, on the other hand, lacks this side effect. While not as potent as intact alpha-MSH, KPV’s absence of side effects makes it theoretically possible to increase dosage levels in most cases to achieve the desired therapeutic effects. The disparity in potency between KPV and alpha-MSH is minimal, at best, as the majority of alpha-MSH’s anti-inflammatory effects are attributed to the KPV segment. Interestingly, the parent molecule seems to excel in suppressing late-stage inflammatory responses. For example, in contact dermatitis, alpha-MSH is more effective at preventing allergic inflammatory responses two weeks after initial exposure, suggesting a potential influence on immune modulation separate from the immediate inflammatory response. Ongoing research aims to elucidate this process further.
Wound Healing
KPV’s role in wound healing and antimicrobial properties
Wound healing is a multifaceted process encompassing inflammatory, proliferative, and remodeling phases. Each phase entails distinct cell populations and cytokine concentrations, providing unique opportunities for intervention. Research reveals that despite variations in skin cell subtypes during each wound healing phase, the majority of these cells express a melanocortin 1 receptor (MC1R), which binds to alpha-melanocyte-stimulating hormone. Consequently, these cells also bind to alpha-MSH analogues like KPV and KdPT. Due to their retention of some alpha-MSH properties while lacking others, alpha-MSH derivatives like KPV offer potential benefits in wound healing. KPV, for instance, retains the anti-inflammatory properties of alpha-MSH but avoids the pigment-inducing activity associated with natural scar formation, particularly in individuals with darker skin. One of KPV’s anti-inflammatory mechanisms involves participation in the innate immune response against two common skin pathogens: Staphylococcus aureus and Candida albicans. Research indicates that KPV inhibits the growth of these pathogens at physiological concentrations, suggesting its potential utility in preventing infections in severe wounds like burns. This sets KPV apart from other anti-inflammatory medications, which often inhibit the body’s ability to combat infections, thus combining anti-inflammatory and antimicrobial activities. KPV serves as a structural model in recent research aiming to replicate its anti-fungal effects in novel therapeutics. The premise is that KPV’s 3D structure underlies its effectiveness as an anti-fungal agent, and replicating this structure may lead to compounds with similar anti-fungal activity but different effects on other biological processes.
Scar Formation
KPV’s role in reducing scar formation and improving wound outcomes
Building on KPV’s benefits in the initial inflammatory phase of wound healing, research also investigates its role in the subsequent stages of wound healing. KPV appears capable of reducing chronic inflammation that contributes to hypertrophic scar formation, such as keloids. This type of scarring involves extensive macrophage infiltration, TNF immunoreactivity, and high neutrophil levels. Administration of alpha-MSH in this context results in smaller scars and a less pronounced inflammatory response. Similar effects have been observed in other tissues, such as the lung and heart. These findings raise hope that KPV could be useful in preventing scarring associated with certain chemotherapy agents. This could not only mitigate cancer treatment side effects but also enable the use of higher medication concentrations for improved cancer treatment outcomes. According to Dr. Didier Merlin, part of KPV’s effectiveness in reducing scar prominence stems from its ability to modulate collagen metabolism. Alpha-MSH and its analogues suppress IL-8 secretion, inhibiting collagen type 1 production. This is particularly significant during the final phase of wound healing, the remodeling phase, as individuals prone to keloid formation and hypertrophic scarring exhibit lower MC1R mRNA expression on dermal fibroblasts.
KPV vs. Alpha-MSH
Comparison of KPV and Alpha-MSH properties and mechanisms
When comparing KPV to Alpha-MSH, it’s evident that Alpha-MSH, although more potent, has a significant drawback – it induces skin pigmentation. This adverse effect has discouraged further exploration of intact Alpha-MSH as a potential anti-inflammatory agent. In contrast, KPV is preferred due to its retention of most of Alpha-MSH’s anti-inflammatory properties without causing side effects. Additionally, KPV’s ease of manufacturing makes it advantageous from both cost and logistical perspectives [15]. Dr. Thomas Luger, a renowned dermatologist and expert in inflammatory skin diseases, has extensively researched and published on KPV, demonstrating its potent anti-inflammatory properties with minimal adverse effects. It’s worth noting that KPV’s anti-inflammatory effects seem to operate through a different mechanism than Alpha-MSH. While Alpha-MSH binds to specific melanocortin receptors, KPV does not. This distinction is supported by mouse studies, wherein blocking MC3/4 receptors, responsible for Alpha-MSH’s anti-inflammatory effects, does not affect the anti-inflammatory actions of KPV. Specifically, blocking these receptors has no impact on the leukocyte migration induced by KPV [16]. Another advantageous feature of KPV is its versatile modes of administration. Research conducted in animal models has demonstrated that KPV can be administered orally, subcutaneously, or via injection (peripheral or central) without causing significant side effects. Recent research has also shown successful transdermal administration of KPV [17]. The ability to administer the peptide through various routes is not just a matter of convenience; it allows scientists to target different areas within the body for treatment.



Reviews
There are no reviews yet.